Case situation
- A patient on her/his 60s
- Recent history of transvenous embolization of a right CCF
- Now, presenting with persistent red-eye, right proptosis and headaches despite the previous embolization.
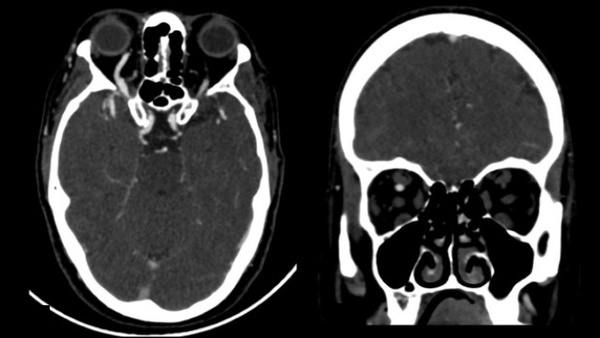
Imaging
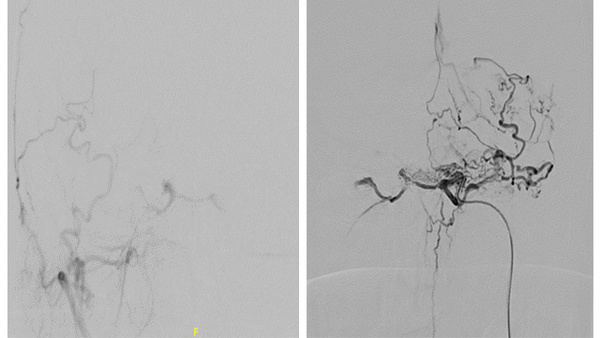
DSA: Injection from right ICA
DSA showed persistent (partially embolized) of the indirect CCF, with feeders originating from both ICAs (meningohypophyseal trunk/ inferolateral trunk), draining into the right superior ophthalmic vein (dilated, but distally thrombosed with no direct drainage into the angular vein).
Right Inferior ophthalmic vein was slightly dilated.
DSA: Injection from left ICA
Lateral view: injection from left ICA
The fistula point/foot of the vein was located at the anterior compartment of right cavernous sinus at the confluence with the ophthalmic vein.
Treatment approach
- Considering that there was no connection with IPS, the first attempt was through the intercavernous sinus from contralateral and the second attempt was performed through direct puncture of right facial vein.
- Several attempts to retrograde navigation into the superior ophthalmic vein were performed, unsuccessful.
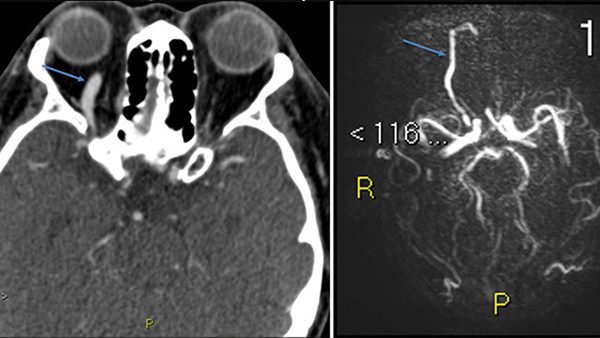
- Images show no direct communication between superior ophthalmic vein and angular vein
TRANSORBITAL PUNCTURE TECHNIQUE
- Considering the morphology of the SOV, the target was to puncture directly the ophthalmic vein/cavernous sinus.
- Puncture was performed as follows: operator handly shifted the patient´s eye laterally, while puncturing the superior/inner lid under roadmap guided (oblique and lateral view).
- Needle progressed following the inner orbit wall until reached the target.
- Arterialized blood refluxed when reaching cavernous sinus. Once there, we exchanged needle using a 0.018´´ Nitrex microwire (Medtronic) placing a 5F radial Sheath (7cm, Prelude IDEAL TM, Merit Medical).
Puncture target: Cavernous sinus/ophthalmic vein confluence
Roadmap: Lateral view for assessing craniocaudal angulation of the needle, and the anterior needle progression
Exchanged the needle using a 0.018´´ Nitrex microwire (Medtronic) placing a 5F 7cm radial Sheath (Prelude IDEAL, Merit Medical) into the ophthalmic vein.
5F sheath was placed into the supero-internal orbit margin.
DynaCT showing the microcatheter through the sheath following the inner wall of the orbit:
An Echelon-10 (Medtronic) was advanced to the fistula point, for coiling and liquid embolic embolization.
DynaCT showing the inner and extraconal microcatheter position within the retrobulbar space, to the inferior third of the superior orbital fissure:
Images showing the coils (Optima, Balt Extrusion) and the Squid-18 (Balt Extrusion) cast at the foot of the vein. Complete occlusion of the CCF was achieved:
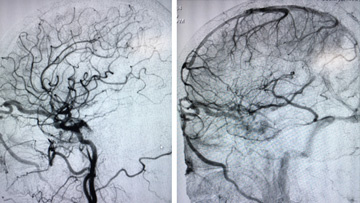
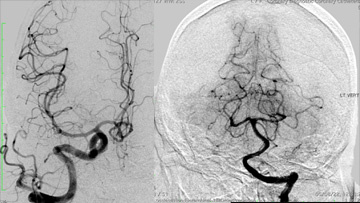
Bilateral ICA runs showing no arteriovenous shunt as result of the complete occlusion of the CCF:
Results
- After sheath removal, we applied a gentle compression over the orbit during 5 minutes, and we placed an orbit coverage with a cold compress (favoring vasoconstriction and anti-inflammatory effect).
- Patient was extubated 3 hours later, with no complication. Cold was applied intermittently during the first 24h.
- Patient was discharged 48h later, with significant less proptosis, without headaches and no visual déficits (photo)