A 70-year-old man presented with insidious and slowly progressive chemosis in both eyes for 3 weeks.
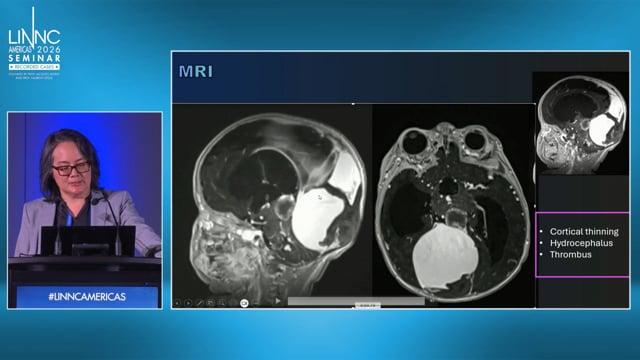
On the advice of the treating ophthalmologist, a brain MRI was performed, which revealed a suspected carotid-cavernous fistula (CCF). A preoperative DSA showed bilateral indirect CCF (Barrow type III) and a grade I dural fistula along left transverse sigmoid sinus. No significant contribution to any of the shunts was observed by either ICA.
You do not have permission to view this object.
During embolization, a 7F short-sheathed 035 guidewire with a 5F spinal slip catheter was inserted into the left IPS though the left jugular vein.
The Marathon microcatheter was passed over the 012 microwire to the opposite cavernous sinus. Under roadmap guidance, Squid12 was injected. The microcatheter was passed back through the inter-cavernous sinus into the ipsilateral sinus. Squid12 was injected under roadmap guidance. Bilateral ECA control angiograms showed complete occlusion of the indirect CCFs.
Subsequently, the left transverse sinus was approached with a microcatheter that was introduced into the transverse sinus. 50 % glue was injected under roadmap guidance with minimal reflux into the cortical veins.
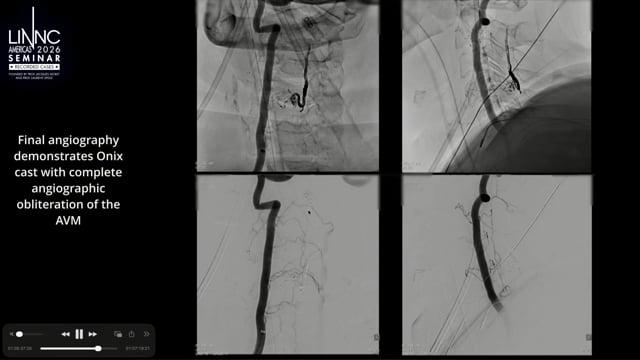
After the procedure, angiography of the left ECA showed complete occlusion of the dural AVF. Chemosis completely resolved after 6 months of follow-up.
Right cavernous sinus cannulation
Embolization of right followed by left cavernous sinus fistulas
Left sigmoid sinus microcatheter injection
50 % glue injection in left sigmoid sinus fistula
You do not have permission to view this object.