The LINNC, it’s spirit. Day 2 and its unique experiences
The atmosphere was filled with anticipation from the moment participants entered the Carrousel du Louvre, especially as the morning sessions began with live cases. For the first time, LINNC featured three simultaneous teams: one led by Gaurav Goel at Medicity Hospital (Gurugram, India), another by Yuxiang Gu at Huashan Hospital (Shanghai, China), and a third by Laurent Spelle at Bicêtre University Hospital (Paris, France).
The second day reflected months of global preparation, as operators welcomed peers into their angiosuites. Each case served as a master class, with every center demonstrating unique approaches to judgment, risk assessment, technique, and courage. I commend all the teams for their dedication.
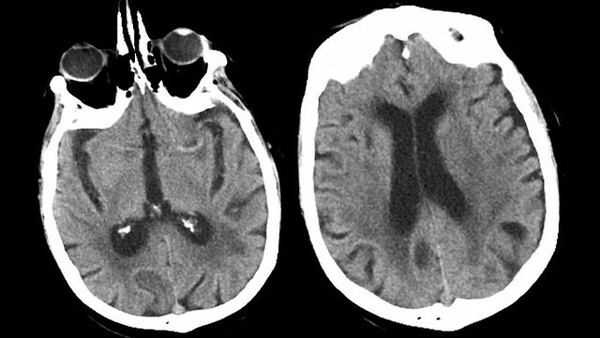
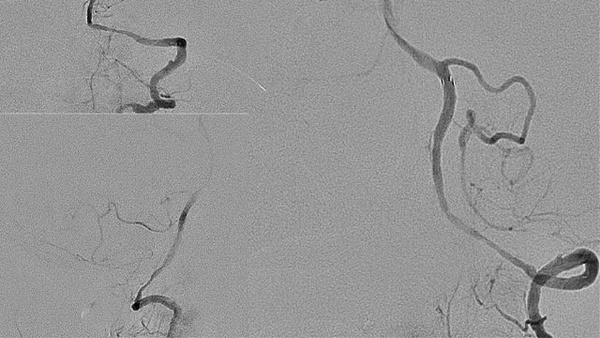
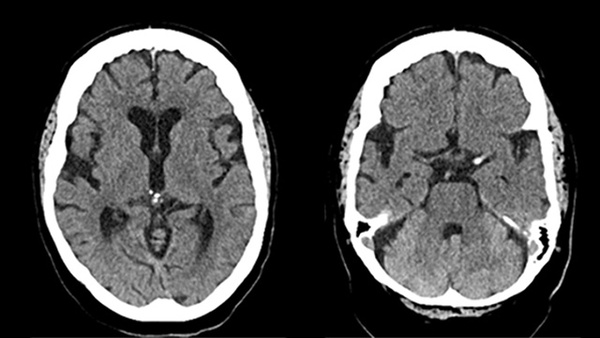
We reinforced key learning points and enriched our discussions by following up on Day 1 cases. Jan Gralla traveled from Bern to further discuss his live-streamed treatment: recanalization of a chronically occluded right internal carotid artery, a procedure that demands significant skill and a deep understanding of vascular hemodynamics.
The objective was to traverse the occluded segment while safeguarding the ophthalmic artery's origin. Gralla emphasized that confirming correct microwire placement was essential; without certainty, he would have opted for bypass, underscoring that patient safety takes precedence over ambition. When the Leo stent did not advance as planned, the team used a balloon-assisted technique, anchoring a PTA balloon to guide the system into the petrous segment. Persistent malapposition and thrombus formation required placement of a balloon-mounted Onyx stent, with Integrilin (eptifibatide) administered for thrombus management, alongside aspirin and ticagrelor. The patient remained stable under strict blood pressure control (systolic ceiling 120 mmHg, ideally near 100) to mitigate hypertension and hyperperfusion risks. Next-day perfusion imaging assessed the MCA territory and ACOM crossflow, and contralateral injections confirmed continued ophthalmic artery perfusion. The open discussion of this complex anatomy was the most instructive moment for me.
Flow Diversion in MCA
At Bicêtre, a right MCA aneurysm was treated with a FRED X (3 × 14/19 mm), deployed from the superior division to the distal M1, achieving precise placement across a challenging bifurcation. Simultaneously, the Shanghai team managed a large ICA aneurysm, prompting a thoughtful discussion on coil-assisted flow diversion, including the decision to add coils and considerations of residual mass effect.
At Bicêtre, flow diversion of an A1-segment aneurysm of the right anterior cerebral artery associated with a fenestration highlighted the importance of proximal support, precise device positioning, and avoiding the dreaded “fish-mouthing” of the proximal border when recapturing the delivery wire. VasoCT and cone-beam CT confirmed the outcome. I noted to Jildaz Caroff that demonstrating the subtlety of this maneuver was a valuable teaching point.
Intrasaccular Innovation & New Devices
At Medicity Hospital, New Delhi, a Contour 11 mm device was used to treat an anterior communicating artery aneurysm. Both Laurent Spelle and Hal Rice emphasized the importance of oversizing, and cone-beam CT confirmed correct placement with preserved flow to both A1 segments. At Bicêtre, a previously ruptured basilar-tip aneurysm, initially treated with a WEB that had compacted, was retreated with a second WEB, against the first and supported by an LVIS EVO (3 × 18 mm).
Wei Ni (Shanghai) introduced the Lattice NEXT, a 48-wire braided Co-Cr flow diverter. The panel discussed vessel selection for deployment, including options from M1 to the ICA, from the left A1 with a Falco braided stent, and the potential use of an e-CLIPs device.
The Wisdom of Restraint
Another follow-up case from Day 1 involved a complex right MCA bifurcation aneurysm. After the microcatheter crossed M2, the exchange was challenging; a stent retriever assisted, but the deployed stent was malapposed and failed to open, with a microcatheter trapped inside. Rodrigo Rivera coiled to protect the dome and made several attempts to advance a balloon through the bifurcation curve. When the stent did not expand as intended, the procedure was appropriately terminated. Flow to the branch was preserved, and the aneurysm was effectively secured.
The patient remains on Agrastat and long-term antiplatelet therapy. Recognizing when to intervene or refrain is itself a mark of clinical mastery.
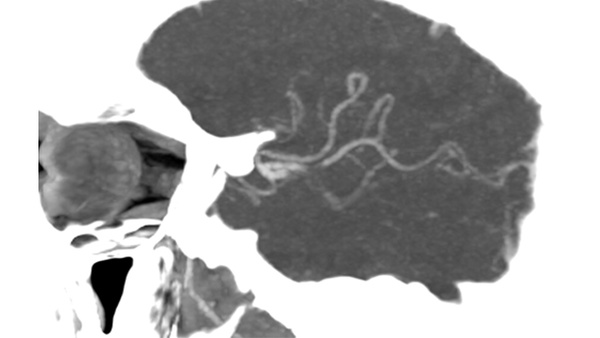
A New Journey — Neuro-Optical Coherence Tomography
Toronto and Vitor Mendes Pereira’s team introduced the most innovative technology of the day. A left ICA paraophthalmic aneurysm was treated with a Surpass Elite, but the highlight was the imaging: neuro-optical coherence tomography (nOCT) revealed a dome wall thickness of 0.019 mm, proposed as a potential surrogate for treatment indication. The prospect of assessing aneurysm wall morphology and thickness as direct predictors of rupture risk marks a significant advancement in neurointervention. Attending LINNC Paris offers the unique opportunity to learn from global experts and engage in meaningful discussions on diverse approaches and strategies. While I can share more about the cases and debates, the curiosity and inspiration at the end of such a productive day is something you must experience with us.
Daniel Vela-Duarte,
St. Mary’s Medical Center | Palm Beach Neuroscience Institute