Patient:
- 34-year-old male patient
- Episodic headaches for 10 years
- No known comorbidities
- Clinically diagnosed with migraine, advised to undergo MRI
- MRI revealed incidental left ICA communicating segment aneurysm
- DSA was performed for further assessment
Bilateral CCA angiograms
3D Spin
Saccular wide neck left communicating ICA aneurysm with anterior choroidal artery arising from its base. The dome of the aneurysm showed microlobulations.
Planned for parent artery reconstruction:
We decided to treat the aneurysm first, as it was multilobulated, with irregular walls, with a reconstruction of the parent artery, as the anterior choroidal artery originated from its base.
The patient received 325 mg of T. Dispirin and 180 mg of T. Brillinta one day prior to surgery, and received subsequent doses as planned.
Hardware
Infinity 80 cm; triaxial combination of CAT5-XT 27-Traxcess ex wire; SURPASS EVOLVE 4.5 x 17 mm
Deployment
From left mid M1 MCA to communicating segment of left ICA; caging the anterior choroidal artery and A1 due to short landing zone
Post deployment - check angiogram
No obvious thrombosis within flow diverter, with good forward flow and patent distal branches
Post-OP Dyna CT
Adequate wall apposition of flow diverter. No thrombosis within flow diverter / proximal branches.
Post-OP:
- The patient had uneventful parent artery reconstruction
- After extubation, the patient was conscious, obeying and moving all 4 limbs
- We received a call from the patient’s attender at about 9:30 pm on the night of the procedure - the patient had collapsed in the washroom and was unable to speak and move his right upper and lower limb
- He had received his nightly dose of brillinta dose in time
- On examination, the patient had global aphasia and dense right hemiplegia, and his BP was 100 / 70
- The patient was shifted for CT / CTA
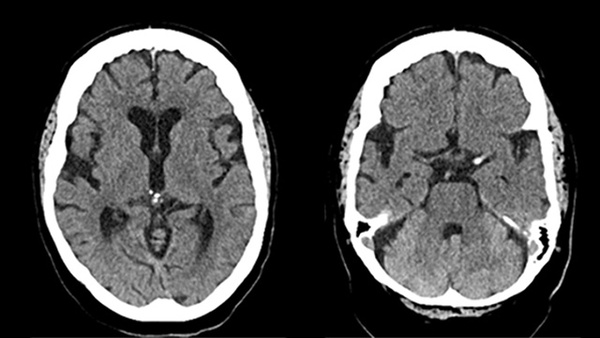
CT brain
Within normal limits. No obvious haemorrhage or infarcts.
Follow-up CTA
Normal filling of the flow diverter and left MCA branches. Perfusion delay in bilateral ACA territories with no obvious filling defects.
- Patient was shifted to cathlab for emergency DSA
- Recovered completely without any intervention within 45 mins (full GCS with no neurological deficits) while being draped for DSA
- Clinical deficit? Postural hypotension vs Thromboembolic event
- Empirically started on IV tirofiban infusion and continued overnight with strict neurological and hemodynamic monitoring in the ICU
- Discharged on POD 3 without any further issues
Clinical deficit? Postural hypotension vs Thromboembolic event
The aetiology was thought to be postural hypotension as the patient felt dizzy when walking to the washroom.
He was unable to stand upright without support and wanted to record the episode on his mobile phone just before he collapsed.
POD 10
- He again presented with an altered sensorium (restless, not obeying but moving all 4 limbs) associated with urinary incontinence
- His recorded BP was 90/60 during the episode and a noradrenaline infusion was started
- His wife reported that this episode immediately followed sexual intercourse
- Working diagnosis – thromboembolic event vs post coital syncope vs post-ictal state
- Shifted to MRI / CTA
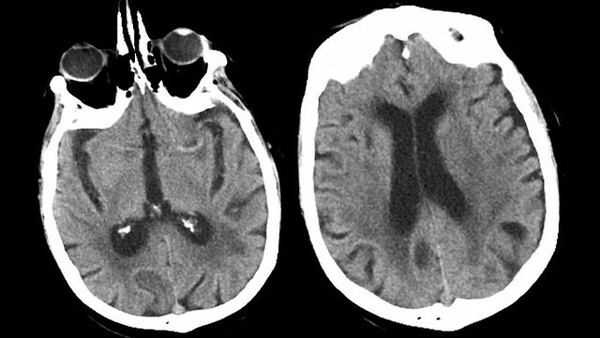
DWI
Multifocal to gyriform DWI changes involving left frontal juxta cortical and insulo-opercular regions with involvement of watershed areas.
ASL
Reduced perfusion signal along bilateral ACA and left MCA territories
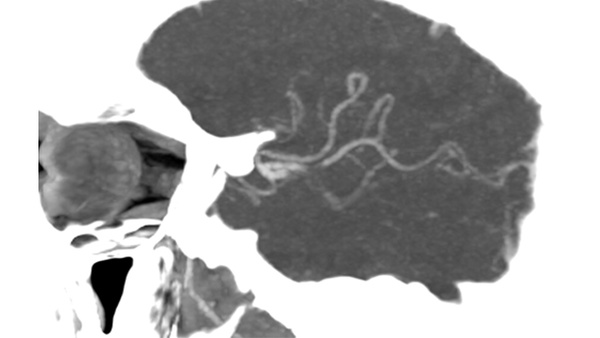
CTA
Filling defect in left A1 ostia. Flow diverter patent. Distal ACA and MCA branches patent.
Management
- Started on Tirofuse infusion along with hemodynamic augmentation
- Gradually improved the following day
- Interval decrease in size of osteoproximal left A1 ACA thrombus
Recurrent Ischemic events
- The acute event was managed without significant long-term complications, but cause of recurrent ischaemic events was still unclear
- Possible cause: decreased oral bioavailability / resistance to Brillinta / hypercoagulable state / migraine induced / hypotension
- Literature review and multidisciplinary discussion including physicians and cardiologists
Does his sexual activity have anything to do with it?
Sildenafil
- One of the cardiologists asked about the use of Sildenafil at the time of intercourse
- His wife was not aware of any medication of this sort, however, did admit that the event occurred after sexual activity lasting more than 45 mins
- Later, the young man aged 35 admitted that he had taken sildenafil, just to have greater experience. He also said that he felt tired and unsteady when walking after sexual activity.
- Sildenafil is a potent vasodilator and can induce severe hypotension
His loss, our peace
After this episode, he stopped taking sildenafil and related drugs altogether, and his clinical course was eventful.
6-month CTA
Complete obliteration of aneurysm (OKM scale D); patent flow diverter with no thrombus or intimal hyperplasia; improved calibre of right A1 ACA and slightly reduced calibre of left A1 ACA
Take-home message
However remote it may seem, ensure that drugs such as Sildenafil are discouraged after parent artery occlusion or parent artery reconstruction caging the origins of major vessels.