The first day of LINNC Paris 2026 was dedicated to hemorrhagic stroke. But rather than being only a thematic deep dive into aneurysms, AVMs, and complex neurovascular decision-making, it felt more like a portrait of a specialty in transition. As always at LINNC, the cases were technically challenging, the discussions direct, and the atmosphere unmistakably witty and international. But beneath the surface of individual procedures, a broader message emerged: neurointervention has reached an extreme level of sophistication and is expanding beyond its traditional boundaries. With that expansion, our need for judgment, humility, and open discussion becomes even greater.
Expanding boundaries beyond hemorrhagic stroke
This was clear from the very first live case, transmitted from Bern: a CSF venous fistula embolization. At first glance, this may seem outside the hemorrhagic stroke theme. In reality, it was one of the most meaningful moments of the day precisely because it showed how the field is widening.
For those of us who treat spontaneous intracranial hypotension, this was a landmark moment. The disease remains underdiagnosed, often disabling, and still poorly understood outside specialized centers. CSF venous fistulas in particular have remained obscure to many clinicians, despite the profound impact they can have on patients’ lives.
To see this procedure on the LINNC stage matters. It matters for patients, whose symptoms are too often misunderstood or minimized. It matters for clinicians, because visibility accelerates recognition. And it matters for the field, because it helps move this condition from a niche interest into the broader neurointerventional conversation. The Bern case was therefore not only a case. It was a signal that even during a day centered on hemorrhagic stroke, the borders of neurointervention are changing.
For many years, neurointervention has been defined mainly by arterial disease: aneurysms, stroke, AVMs, stenosis. These will remain central, and Day 1 clearly reflected that. But the venous side of the field is rising. CSF disorders, venous hypertension, fistulas, pressure-related syndromes, and other emerging indications are increasingly becoming part of our procedural identity. The first case of the day captured that transition very clearly.
AVMs and the persistent challenge of indication
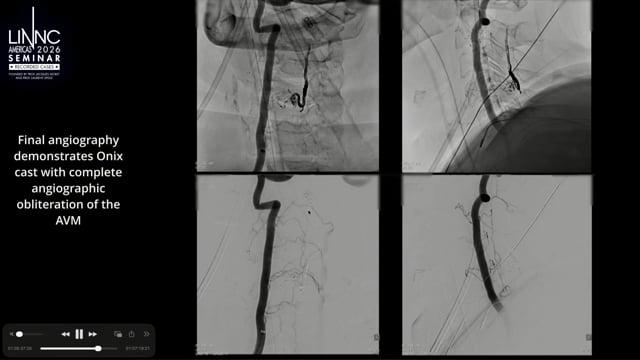
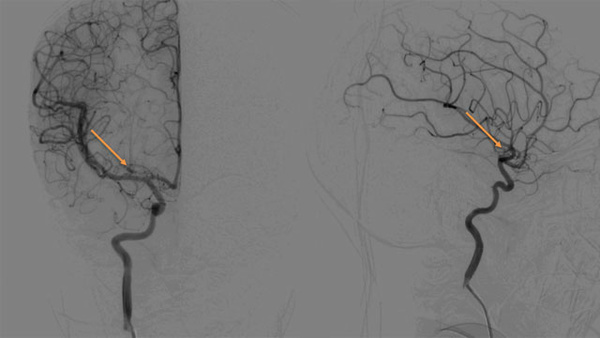
The live AVM case from Bicêtre brought the discussion back to one of the oldest and most difficult questions in hemorrhagic stroke prevention: not whether we can treat, but whether we should, and how. AVMs have always forced us to confront uncertainty.
ARUBA, TOBAS, MARS, and other efforts have helped frame the debate, but they have not eliminated the nuance of individual decision-making.
This lesion was asymptomatic, but had changed on MRI. That immediately raised the real questions: should it be treated? If yes, how? Embolization, surgery, radiosurgery, or continued observation?
The value of the case was not that it offered a simple answer. It was valuable because it showed how complex the answer remains. As our tools improve, decision-making does not necessarily become easier. In some ways, it becomes harder. When treatment was impossible, the decision was made for us. Now that treatment is often technically possible, we must be much more precise in deciding when it is justified.
Multidisciplinary exchange and operator experience
This dynamic was reinforced by the format of the meeting. The “Voices in the Audience” initiative felt like more than a stylistic change. It reflected something important about how complex cases should be discussed. Difficult cases benefit from more thoughtful perspectives, not fewer.
The field is at its best when discussion is not confined to the panel desk, when disagreement is welcomed, and when experienced operators can think aloud from different positions in the room.
Guilherme Dabus’ complication presentation offered the necessary counterweight to the enthusiasm generated by innovation and technical bandwidth. Aneurysm treatment may be familiar territory, but familiar does not mean safe. Things can deteriorate quickly, even in cases that appear routine. A procedure can move from controlled to critical in seconds.
The complete carotid revascularization case from Bern was another excellent demonstration, and again the central issue was indication. Although not a classic hemorrhagic stroke case, it belonged in the same intellectual space: complex cerebrovascular disease where technical possibility must be weighed against clinical necessity. There are procedures at the edge of standard practice where the question is not only whether we can perform them, but whether the patient truly benefits. The case also highlighted something very real in daily practice: despite having an extraordinary number of devices, we still do not have a dedicated solution for every scenario.
Evolving therapeutic strategies in hemorrhagic stroke
Riitta Rautio’s presentation on coil embolization of the middle meningeal artery for chronic subdural hematoma was timely and very much aligned with the hemorrhagic stroke theme. MMA embolization continues to grow rapidly, and long coils are being extensively used and studied in the United States, where this approach has gained significant traction. It is now increasingly entering European practice as well, adding another option to a space that is evolving quickly.
Coil embolization is not the answer for every chronic subdural hematoma, and it should not be presented as a panacea. But in selected cases it is an extremely valid treatment. As the indication matures, the question will likely move from “does MMA embolization work?” to “which embolic strategy is best for which patient?”
The next case from Bicêtre continued the theme of increasing sophistication in aneurysm treatment. Intrasaccular devices are multiplying, and each has specific behavior, sizing rules, marker considerations, and deployment nuances. This matters. As we acquire more options, we must also acquire deeper device literacy. The operator must understand not only how to deploy a device, but how it behaves, how it interacts with the aneurysm, and how it can fail.
Innovation, evidence, and expanding possibilities
In the afternoon, Frederic H. Moll’s lecture on surgical robotics widened the lens. It was inspiring to hear from a physician-inventor and entrepreneur who helped define a field outside neurointervention, speaking to a specialty that has always been forward-looking by nature. Robotics, automation, simulation, imaging integration, and artificial intelligence are no longer distant concepts. They are part of the environment in which procedural specialties will evolve.
The question is not whether technology will enter neurointervention more deeply. It already is. The real question is how we will shape it, and whether we will remain clinicians first while adopting tools that may change the mechanics of our procedures.
The left pericallosal aneurysm case from Chile was an elegant example of modern aneurysm decision-making in hemorrhagic stroke prevention. WEB or flow diverter? Both options could be discussed. Flow diversion was chosen, and the execution was excellent. But again, the most interesting part was not only the result. It was the debate. A single clinical problem may now have several reasonable solutions. This is progress, but it is also difficult. More options improve patient care, but they also increase the cognitive burden on the operator.
Day 1 closing remarks and key takeaways
The day closed with two very complex aneurysm treatments, including a basilar tip remnant from Bicêtre and a challenging MCA bifurcation aneurysm from Chile. These were the right cases to end on because they captured the central dilemma of contemporary hemorrhagic stroke intervention. We can now treat almost everything. But when should we? When should we touch, and when should we leave alone? When is complexity justified, and when is restraint the more sophisticated intervention?
Day 1 of LINNC Paris 2026 did not provide simple answers, and that is why it was valuable. It showed hemorrhagic stroke intervention at its most sophisticated, but also a field entering a broader new era. Venous intervention and CSF disorders are becoming more visible. Robotics and automation are approaching. Aneurysm devices are becoming increasingly refined. The range of what we can treat is expanding.
But progress does not make humility obsolete. It makes it more important. The future of neurointervention will be shaped by innovation, new indications, and better devices. It will be protected by judgment, preparation, restraint, and honest discussion. That, to me, was the real message of the first day.
Emanuele Orru
Lahey Hospital & Medical Center
Burlington, Massachusetts, USA