ABC WIN 2026 felt less like a traditional scientific meeting and more like a snapshot of a field in transition.
Neurointervention is clearly moving beyond the pursuit of isolated technical success toward a broader, system-level optimization of care.
What struck me most this year was the growing centrality of venous disorders and CSF leak syndromes, fueled by hybrid imaging strategies and increasingly mature endovascular techniques.
At the same time, advances in flow-diverter design, intraprocedural imaging, artificial intelligence, and robotics are reshaping, not incrementally, but fundamentally, how we think about device–vessel interaction, procedural safety, and operator performance.
This is therefore not a comprehensive report, but a deliberately subjective reading of the messages that, in my view, best capture where the field is heading.
Venous pathology
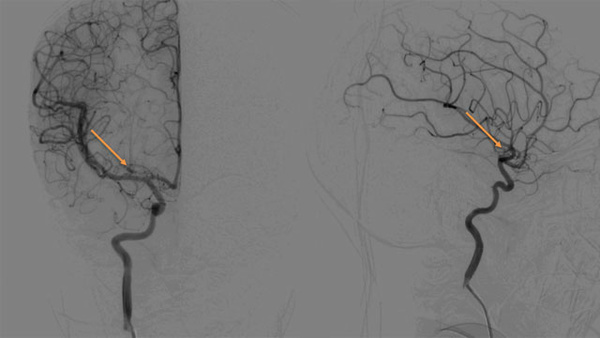
Dr Shapiro : Venous pathology session
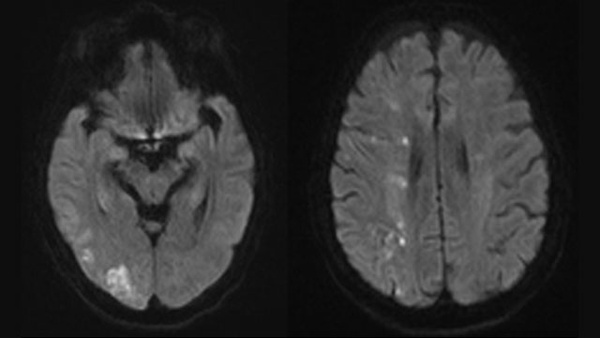
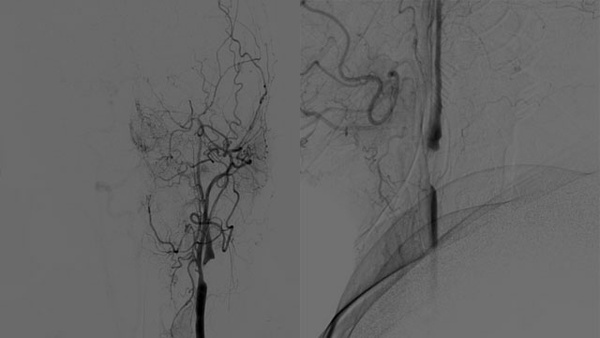
The venous session was, to me, one of the clearest indicators of this shift. Dr. Shapiro’s DSA-based analysis of venous drainage in IIH offered a convincing pathophysiological framework, suggesting that reduced venous outflow redundancy may act as an independent risk factor. This concept elegantly explains why IIH may develop in low-BMI patients while sparing many individuals with high BMI, and challenges some of our traditional assumptions.
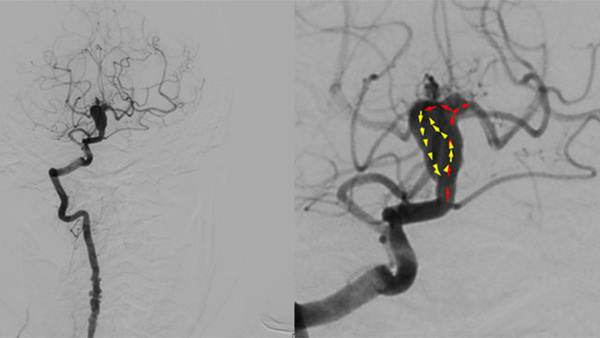
Dr. Costalat emphasized the potential risks of transverse sinus angioplasty and presented cases in which residual post-stenting stenosis resolved spontaneously within weeks—an important reminder to avoid overinterpreting immediate angiographic results.
The discussion around venous-specific stents was particularly revealing. Dr. Bricout’s argument in favor of lower radial force—to potentially reduce post-procedural headaches—and longer stent designs compatible with smaller delivery platforms resonated strongly with everyday clinical experience.
Experiences shared around venous thrombectomy converged toward a clear and somewhat uncomfortable conclusion: our current tools are not yet good enough. In this context, Professor Cognard’s announcement of an upcoming French randomized controlled trial felt like a necessary and timely step forward.
MMA embolization for chronic subdural hematoma
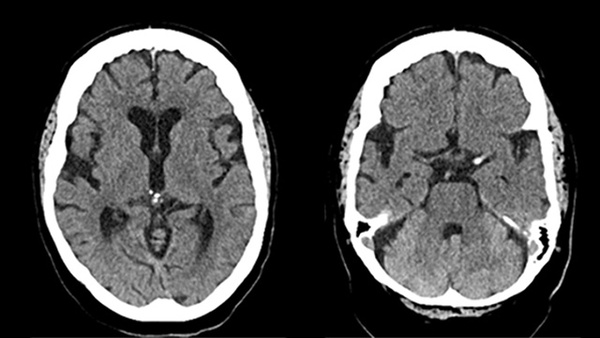
Dr. Weng’s post hoc analysis of the MAGIC-MT trial reinforced a message that is becoming increasingly difficult to ignore. MMA embolization is not a universal solution, but a powerful one when applied to the right patients. The demonstrated benefit in high-density cSDH—and the absence of superiority in others—strongly supports the ongoing transition toward imaging-driven informed patient selection.
Dr Weng : Post hoc analysis of the MAGIC-MT trial
Iatrogenic procedural contamination
One of the most intellectually unsettling presentations came from Dr. Hohenstatt, who addressed the largely overlooked issue of iatrogenic contamination during neurointerventional procedures. Beyond particulate debris, chemical contamination—particularly PFAS—emerged as a potentially greater and underrecognized risk.
Dr Hohenstatt : Iatrogenic procedural contamination
The demonstration of ubiquitous micro- and nanoplastic contamination and PFAS levels far exceeding safety thresholds, especially during mechanical thrombectomy, forces us to confront an uncomfortable reality: procedural safety may depend not only on technique and experience, but also on material science. This is an area where closer clinician–industry collaboration is no longer optional.
Lessons from ISAT
Professor Molyneux’s lifetime achievement lecture provided a rare moment of perspective. By synthesizing decades of work from ISAT 1 and ISAT 2, he reminded us how evidence, when patiently accumulated, can genuinely reshape practice.
ISAT 2 confirmed the non-inferiority of endovascular treatment across aneurysm subtypes—including wide-neck MCA aneurysms—while demonstrating clear advantages in terms of vasospasm-related DCI reduction, much shorter length of stay, and fewer needs for CSF diversion. Rebleeding appeared very low and equivalent in both groups.
Dr Molyneux : ISAT 2
His conclusion was striking in its clarity: when endovascular treatment is anatomically feasible with available devices, it should be the treatment of choice.
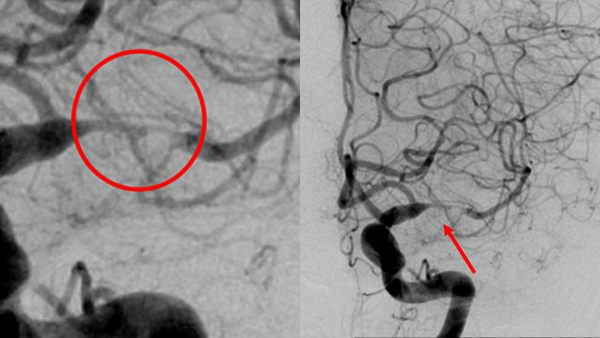
Flow-diverter braid deformation
Dr Bernava : Radial load-induced braid collapse in flow diverters
Finally, multiple presentations addressed the current limitations of flow-diversion technology, particularly braid deformation.itional assumptions.
Rather than signaling a plateau, these discussions highlighted a field that is actively interrogating its own weaknesses.
The diversity of proposed solutions—from mechanical redesign to surface modification and advanced intraprocedural imaging—suggests that flow diversion is entering a phase of refinement rather than reinvention.
Taken together, these reflections represent my personal synthesis of the scientific and clinical signals emerging from ABC-WIN 2026, shared here with the LINNC Online community.
Reported by
Jildaz Caroff