Patient
- 79-year-old female, mRs 0. Known to have DM II as AF for which she takes Apixaban. Recent technical fall resulted in acute SDH. Later evolved to cSDH with significant mass effect which necessitated halting Apixaban and a Burr hole was performed.
- One month follow-up NCCT demonstrated significant Lt hemispheric mixed cSDH.
PRE – Embolization CT
Management
The neurosurgery team decided not to perform another cSDH evacuation due to the failure of the first procedure and the need to resume anticoagulation as soon as possible.
Radial approach using RISTTM system was performed due to patient preferences.
Equipment:
- 7 Fr radial sheath
- 7 Fr RISTTM catheter
- SonicTM 1.2 25
- HybridTM 007 microwire
- OnyxTM 18
Technique- Radial approach
Performed using dedicated RISTTM radial sheath.
After careful insertion of the sheath, local Nitroglycerin was given as well as systemic Heparin.
DSA run was performed to verify no adverse effects and to obtain DSA roadmap.
Technique- LICA access
Due to type iii arch, SimTM II select was used to access both LCCA, but also the distal LECA, which was difficult for access by a 038 GlidewireTM.
Due to its excellent trackability, the RISTTM was placed at the distal ECA.
Technique- MMA access
SonicTM 1.2 microcatheter was advanced over HybridTM 007 to the dominant anterior branch.
The small posterior branch was not accessed due to its small size. Proximal occlusion was dangerous due to proximity to the foramen spinosum and petrosal branch.
0.4cc OnyxTM 18 was injected until the reflux reached the proximal portion of the first detachment point.
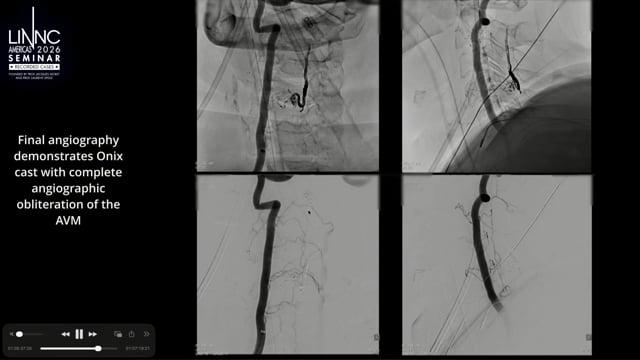
Technique- Control DSA
The dominant branch of MMA was embolized while preserving the important petrosal branch.
Further management
Patient was discharged the next day neurologically intact.
Apixaban was resumed.
The patient will come back in 6 weeks with NCCT.
This case is sponsored by Medtronic.