Definition
Intracranial DAVFs are rare, acquired pathological connections between dural arteries and dural venous sinuses, meningeal veins, or cortical veins.
Absence of nidus on angiography.
Arterial supply: branches of the external carotid artery, meningeal branches of the vertebral artery, tentorial branches of the internal carotid, or small pial branches of cerebral arteries.
Venous drainage: anterograde into dural sinuses or meningeal veins, or retrograde into dural sinuses, leptomeningeal veins, or cortical veins.
Risk factors: venous sinus thrombosis, meningitis, sinus infection, previous surgery, hereditary hypercoagulable states, and trauma, and most of them are idiopathic.
Signs and symptoms:
- carotid-cavernous region DAVFs: the clinical triad of proptosis, chemosis, and bruit, and finally with decreased visual acuity and possible blindness.
- DAVF of the petrous region of the transverse sinus: pulsatile tinnitus or headache.
- malignant presentations: intraparenchymal, subarachnoid, and subdural hemorrhage, which is seen in patients with retrograde cortical drainage DAVFs.
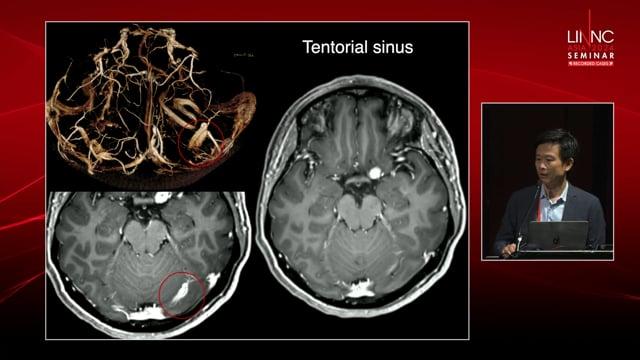
- locations and hemorrhage; 75 % of DAVFs manifesting with hemorrhage were tentorial, and about one third had an associated venous varix.
Classification:
Patient
- 58 y/o man with sudden onset headache, vertigo and imbalance
- GCS: 15
- FND: ataxia and impaired cerebellar test
- Medical Hx: HTN
- Social Hx: opium and smoker
- Drug Hx: captopril
- Brain CT: cerebellar hemorrhage more prominent in vermis and intra-ventricular hemorrhage
- Brain CTA: prominent vascular marker in posterior fossa and tentorium
- DSA: complex cranial dural AVF; feeder from meningeal branch of left vertebral artery
- Right Posterior inferior cerebellar artery (PICA)
- Occipital and MMA branch of external carotid artery
- Drain to vermian vein and transverse sinus
Plan
Selective catheterization of feeder and embolization on fistula
Initial brain CT: cerebellar hemorrhage
Brain CT angiography: prominent vascular marker in posterior fossa
Sign of hemorrhage in posterior fossa and 3rd ventricle. Prominent vascular marker around occipital surface of cerebellum and tentorium.
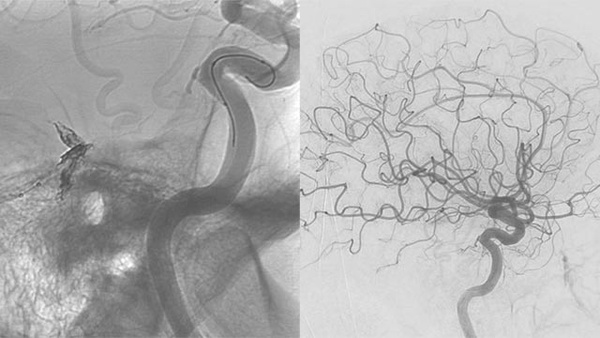
DSA: Angiography from left vertebral artery showed small fistula from meningeal branch of vertebral artery
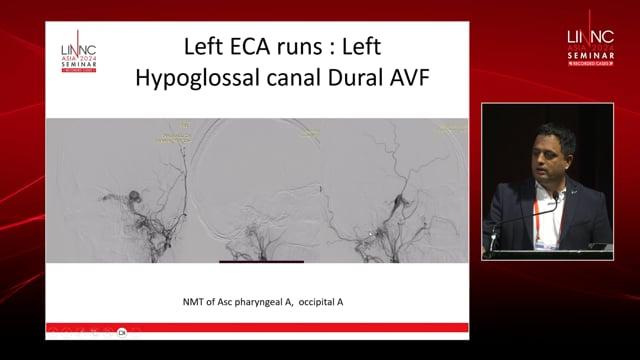
Angiography from ECA with prominent fistula from occipital artery
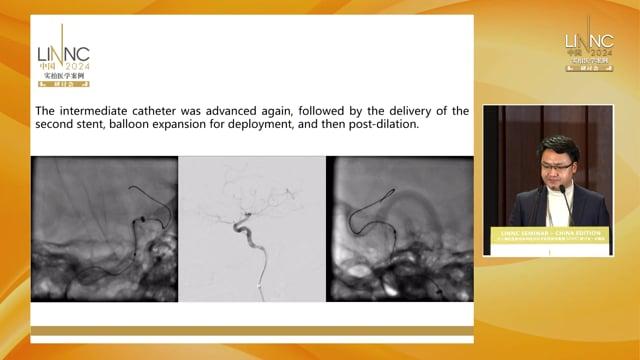
Selective catheterization of occipital artery
Glue injection, occipital artery
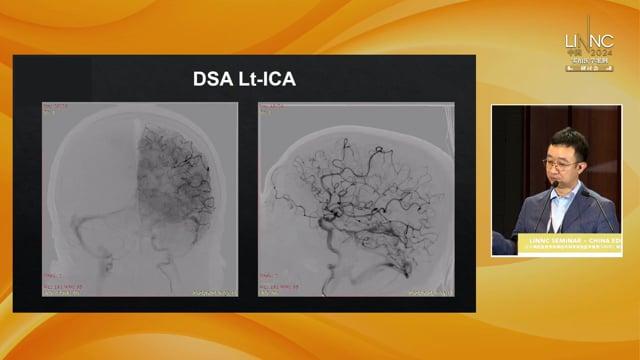
Angiography from ECA and fistula from MMA
Selective catheterization and embolization of fistula
ECA angiography after embolization of fistula
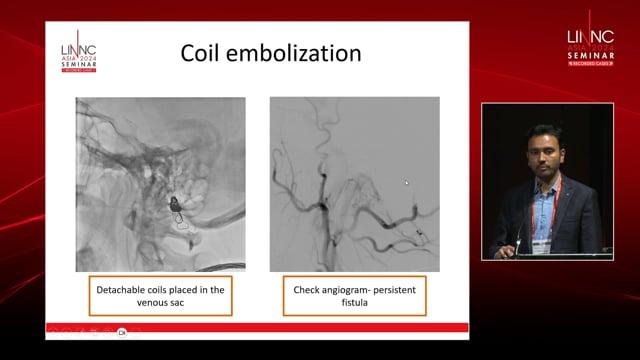
Angiography from right vertebral artery and prominent PICA artery and fistula to vermian vein
Selective catheterization of PICA artery and embolization of fistula from PICA
Angiography of right vertebral after fistula embolization
Post-operative CT scan. Patient discharged 2 days after embolization without new deficit.
Endovascular embolization is generally the first-line treatment for DAVF.
Prior to embolization, a complete understanding of the fistula angioarchitecture is mandatory. The feeding arteries, the fistula connection point, the venous drainage pathways, and the direction of venous flow must be identified. Endovascular approaches are performed by arterial, venous, or combined methods, depending on the location and anatomy of the fistula.