Welcome to LINNC 2025 – Day 1 Highlights
We kicked off LINNC 2025 with a warm welcome from the Course Directors and an exciting faculty lineup.
Let’s start from Kazakhstan with the team led by Dr. Mynzhylky from the National Hospital of Almaty.
The first live case was a 67-year-old male with diffuse intracranial atherosclerosis and a right extracranial carotid stenosis who underwent a combined treatment session: right carotid stenting followed by management of a 5 mm ACom saccular aneurysm. The aneurysm was treated via left carotid access using an ipsilateral ACA stent-assisted coiling technique—necessary due to a hypoplastic right A1 segment. This sparked an engaging discussion: would an intrasaccular device have been a better choice? Could it reduce procedural morbidity, especially in a patient requiring 6 months of DAPT? Pr. René Chapot and the panel fueled the debate, highlighting the balance between procedural simplicity and patient comorbidities. Despite the complexity, the procedure was flawlessly executed—bravo to Dr. Mynzhylky and his team! Final takeaway from Dr. Lanzino…Always aim for the lowest morbidity strategy that effectively prevents rupture—simplicity always wins!
Let’s move to the first Innovation Session where Pr. Pierot presented the first randomized study on surface-modified flow diverters—the COATING trial—exploring the use of Glycocalyx-coated stents designed to reduce thrombogenicity. The trial compared coated stents under single antiplatelet therapy (SAPT) vs. uncoated stents under dual antiplatelet therapy (DAPT), enrolling 171 patients (83 SAPT vs 88 DAPT).
The interim results at 1 month? No significant difference in thromboembolic or hemorrhagic complications! A significant step forward toward SAPT—but we still wonder: how long can thromboembolic risk persist? Will SAPT affect long-term in-stent stenosis rates? We should still wait to have an answer to these questions.
The first case from Bicêtre was a small aneurysm in a tricky spot! A 49-year-old woman with multiple cardiovascular risk factors had an incidental 4 mm wide-neck left MCA aneurysm at a trifurcation point. The treatment strategy by Dr. Mihalea was a laser-cut stent and coils—a decision broadly supported by the faculty. Although braided stents offer better visibility, the anatomy here favored the laser-cut approach.
Handy tip from the case? Just make sure not to exit through the stent struts after deployment and… it is not always necessary to pass through the struts of the stent to deploy the coils!
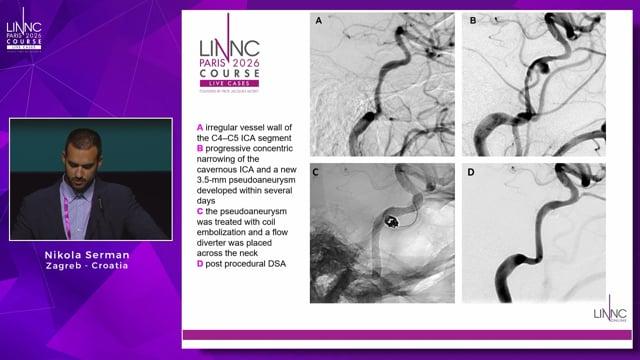
Now is the time for the complications corner… “When the Unexpected Happens”, presented by Dr. Gralla, who kindly shared a complex case of stroke-related complications. A 72-year-old with a cervical dissection and sub-carotid T occlusion. After two thrombectomy passes, a carotid rupture occurred. The ophthalmic segment was coiled, but the clot migrated distally, resulting in a massive left hemispheric infarct. Retrospective imaging evaluation showed a previously undetected small ophthalmic aneurysm, masked by the dissection. Thanks to Dr. Gralla for sharing with us this difficult case.
Back to Almaty for a challenging case to treat a ruptured posterior circulation AVM in the eloquent mesial-temporo-occipital region, with multiple flow-related aneurysms, including one intra-nidal.
While there's no consensus on the timing of ruptured AVMs treatment, the panel largely agreed that in this case, where the bleeding source was clearly identifiable, acute embolization was the right move. Dr. Mynzhylky and his team went for a curative embolization using multiple microcatheters, balloon-pressure cooker technique from the arterial side, combined with a venous approach. A heated debate followed, including questions about when can we be confident the entire nidus is occluded? When should we stop injecting embolic agent? This was a technically complex, impressive curative case, ending the session on a high note. Congratulations on this outstanding case!
Dr. Psychogios presented the much-anticipated results of the DISTAL trial, shedding light on the most effective techniques for distal vessel recanalization in acute stroke treatment. The findings suggest that the use of smaller aspiration catheters is pushing the field in the right direction, showing very promising TICI reperfusion results in distal occlusions.
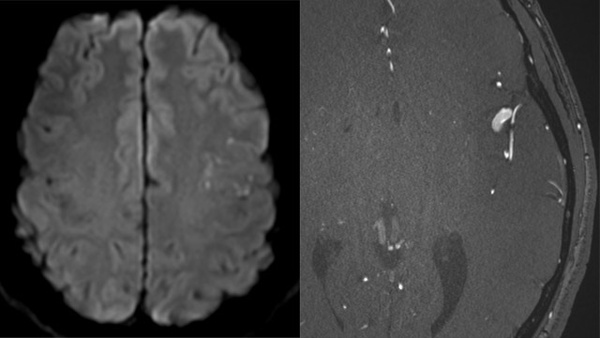
Following that, Dr. Michihiro impressed the audience with an in-depth analysis of dural membrane micro-anatomy using Cone-Beam CT. The detail in these images was exceptional—the microvascular architecture was clearly visualized, providing all the information needed to plan targeted treatment for chronic subdural hematomas. Truly spectacular imaging, opening new horizons in minimally invasive hematoma management!
The second case from Bicêtre was led by Pr. Spelle. This involved a 74-year-old woman with a history of hypertension and dizziness, found to have a 10 mm unruptured ophthalmic aneurysm with a frightening bleb on the sac, set within an irregular, dysplastic right carotid artery. Pr. Spelle chose a flow diverter stent plus coils, delivered via radial access. During the discussion, Dr. Gralla raised an interesting question: Why not just coil the bleb instead of treating the entire vascular segment?
An intriguing idea—but, as we all know, not always a piece of cake, as suggested by Pr. Moret!
One critical issue raised: What if the stent shows distal malposition due to the challenging anatomy? Should we reconstruct the distal vessel, or leave it? That’s the question—and the debate is still open.
Lunch break’s over… Let’s dive into the afternoon!
The afternoon session kicked off with another case from Bicêtre Hospital, where Pr. Spelle took on a challenging AComA aneurysm recurrence in a 52-year-old male—previously treated with coils in the acute phase. This time, the strategy was a flow diverter. The panel noted that an intrasaccular device could also be a solid and maybe easier alternative in such case. The real key to success here? A pre-shaped, dedicated microcatheter, which made the catheterization of the recurrent A2 segment both feasible and elegant. Despite the technical difficulty, the case was beautifully handled.
Next up, the team from Medellín, Colombia, introduced by Dr. Jankowitz, presented a right PComA aneurysm measuring around 10 mm with a 6 mm wide neck and a second smaller wide neck aneurysm on the opposite left PcomA. The plan: treatment of both aneurysm in the same session!! A brand new-generation of intrasaccular device used—an exciting two-in-one case to follow closely!
Last case of the day from Bicêtre was a challenging Pericallosal Aneurysm managed by Dr. Ikka, involving a 67-year-old man with an incidental 9 mm left pericallosal aneurysm, characterized by an irregular sac and a left azygos ACA configuration. The chosen strategy: a flow diverter stent delivered via radial access. The main challenge? The right ACA originates directly from the aneurysmal sac, adding a layer of complexity to both the anatomy and the treatment planning. Let’s dive into it!
Closing the day from Medellin, with a complex multi-aneurysm case in an 81-year-old patient with severe headache. A 5 mm right PcomA aneurysm, the largest of the three plus two smaller aneurysms at the left MCA. The treatment plan was tailored to each lesion: intrasaccular device for the right PcomA aneurysm via radial access and flow diverter for the left MCA aneurysms through a femoral approach.
A well-executed, single-stage multi-strategy approach—an example of how anatomy-driven treatment planning can make the difference in a potentially more fragile patient.
This was a truly enriching first day at LINNC 2025—packed with complex anatomy, evolving technologies, and thought-provoking debates that should remind us…that this is just the beginning!
See you for Day 2—more challenging cases, cutting-edge innovation, and insightful discussion await at LINNC 2025. In the meantime, enjoy the beautiful Paris by night!
Valerio Da Ros
University Hospital of Rome Tor Vergata
Rome, Italy