- 60-year-old, Right handed male
- Late window: last seen well 07:30hrs, in-house referral 17:00hrs =9.5 hours post onset
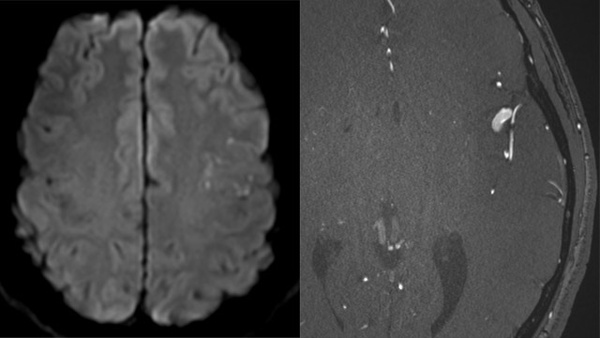
- Favourable non-contrast CT; ASPECTS 8
- CTA: Tandem, Left M1 MCA / ICA occlusion – mixed calcified/soft plaque
- Large syndrome, hemiparesis, NIHSS: 16
- No thrombolysis – out of window
Notification received via RAPID mobile - Left distal MCA occlusion (circle)
CTA shows tandem occlusion
CTP Summary – large potentially salvageable ‘penumbra’ (green) v small core (pink)
CTP Summary (2)
Favourable Hypoperfusion index, suggests good collaterals
Thrombectomy Setup
- General Anaesthesia – complex case
- Consent 4; lacks capacity to consent
- DSA: No antegrade ICA flow
- Terumo 035 wire and Neuron 5Fr Select catheter via Walrus balloon guide
- Difficult lesion to cross, no evidence of arterial dissection
- Aspiration below lesion through Walrus Balloon Guide (low position); thrombus delivered
- Diagnostic catheter switched for React 071 device over exchange 035 wire to maintain access
Initial Angiography- tandem occlusion (arrows)
Primary Target
Left M1 MCA
Initial perfusion: TICI 0
No of passes: 2
Technique: Combined Aspiration (REACT™ 71) and Solitaire™ X (Aspiration catheter left in situ to maintain access)
Stent: Solitaire™ X 6*20mm
Microcatheter: Trevo Trak™ 21
Microwire: Synchro™ 14
Final perfusion: TICI 3 but embolization to new territory
First Pass- Secondary MeVO, TICI 0
Second pass, MCA TICI 3, MeVO remains
Secondary Target
Left ACA (embolic occlusion, ENT)
Headway 17, Traxcess™ Mini 007 wire with J for safe distal navigation. Microcatheter injection to understand distal anatomy prior to stent placement
No of passes: 1
Technique: Combined Aspiration and Stent (*1)
Final perfusion: TICI 3
Microcatheter injection (tip arrow) - Stent deployed (arrows)
Stentriever deployed (arrows)
TICI 3, minor ACA spasm
Left ICA Stent and Antithrombotics
- Left internal carotid artery- appearance concerning for re-occlusion
- Eptifibatide (Integrillin) bolus IA and infusion 24 hours prior to DAPT conversion
- Wallstent™ Carotid Stent deployed across the lesion 9mm*40mm
- Aviator™ Balloon angioplasty 6*20mm throughout stent
- Eptifibatide (Integrillin) bolus IA and infusion 24 hours prior to DAPT conversion
Stent (arrows) deployment through BGC
24 hour NCCT- small volume infarction




")


 v small core (pink)")
 - Favourable Hypoperfusion index, suggests good collaterals")
")
")




 - Stent deployed (arrows)")
 - Stent deployed (arrows)")
")
")


 deployment through BGC")
 deployment through BGC")